
Since the evidence of the iStent inject is attaining better outflow via improved access to the collector channels, surgeons may wonder about the relative merits of the iStent
inject compared to the Hydrus, which should provide even greater access to the
channels, at least in theory.
“Some surgeons might prefer the iStent inject because it’s a ‘stealth’ device and
the least-tissue-disruptive canal intervention.”
The concept that might favor an iStent approach: you put in two minimally tissue-
disruptive, extremely focal stents, leaving 98 percent of the canal normal, but
improved from the phaco effect. There’s room for more than one canal device, just
as we have multiple IOL platforms and phaco machines. “Ultimately, the device
that surgeons favor may depend on what long-term data shows in a large
population of patients.”
Conclusion
“iStent inject is to be seen even easier than the Hydrus. I think the iStent inject
will replace the original iStent very quickly.”
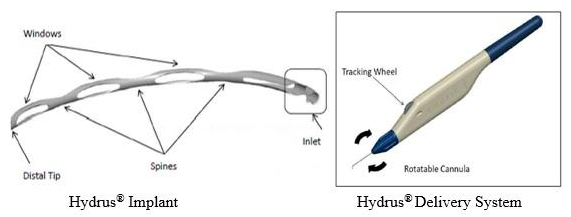
“On the other hand, many surgeons will like the Hydrus design, and the fact that
you can directly verify that it’s exactly where you want it to be in the canal
because you can see it through the translucent inner wall.”
“In the Hydrus, we’re manipulating 8 mm of the canal in a very important region,”
“As a result, there could be some fibrosis over time that might not occur with a very
stealthy implantation like the iStent inject, which is very tissue-friendly and
maintains the normal architecture of the canal as much as possible. The data
clearly show that cataract surgery alone improves physiologic function, so one
might argue that it makes sense to disrupt the tissue as little as possible while
augmenting outflow.
Conclusion
The Hydrus has a lot of potential,” says Dr. Samuelson. “The data from the
HORIZON trial, which is the pivotal U.S. trial for Hydrus, was tremendously
favorable—probably the best MIGS data that we’ve seen to date, in terms of the
important combination of sustained efficacy and safety. The advantage of
Hydrus is the tri-modal mechanism. First, it provides a direct inlet into the canal
because the tail end of the Hydrus resides in the anterior chamber. Second,
the main body of the Hydrus, the remaining 7 mm or so, sits within the
canal, maintaining its patency. Third, it also tensions the canal tissue, improving
physiological outflow.” According to Dr. Crandall, a recent trial that compared the
Hydrus to the iStent used the original iStent, not the iStent inject. “If the Hydrus
did better than the single iStent, that shouldn’t be a surprise; the Hydrus
accesses at least 90 degrees of the canal, so its odds of accessing one or
more outflow channels is much greater.